

 English
English 



















































































































































































































































































































































Hantavirus Quarantine Pressures US Health Trust

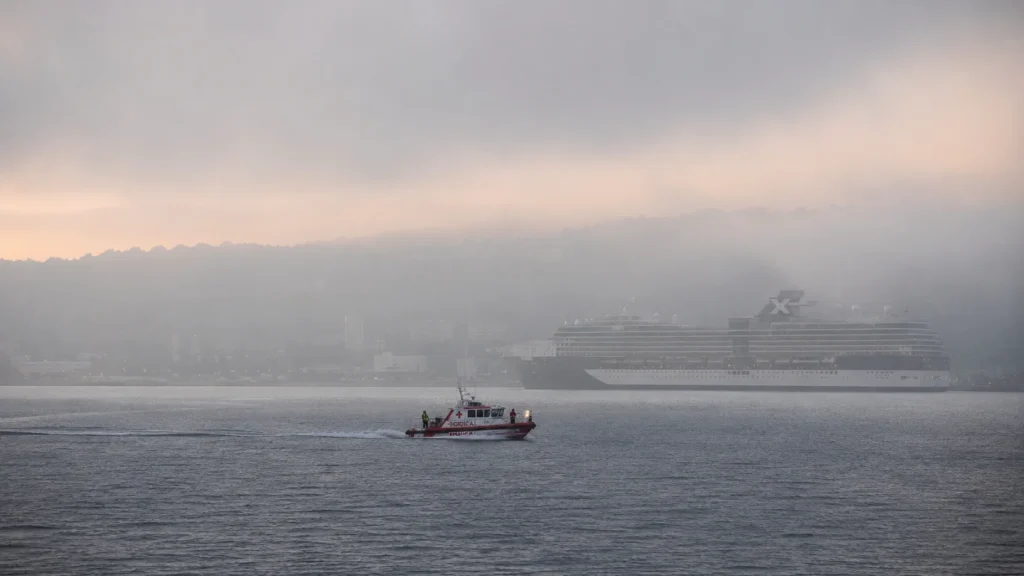
The US hantavirus response entered a new phase after Dr. Stephen Kornfeld, a passenger from the MV Hondius cruise ship, tested negative following an earlier “faintly positive” result and left a Nebraska biocontainment unit on 14 May 2026. Yet quarantine monitoring continues for exposed passengers across multiple states. The episode now tests how far American public health systems can rely on voluntary compliance, institutional trust, and post-pandemic containment strategies.
The Question Behind the Quarantine
A negative test usually ends a medical scare.
This time, it didn’t.
The CDC still encouraged exposed passengers from the Hondius expedition cruise to remain under observation because Andes hantavirus carries a long incubation window and documented person-to-person transmission risk. That decision reveals something larger than one cruise outbreak.
Modern outbreak medicine increasingly treats exposure itself as operational risk.
After COVID-19, health agencies no longer wait only for confirmed illness. They map movement patterns, contact chains, travel routes, and behavioural compliance. One symptomatic traveller now activates hospitals, airport tracing systems, quarantine facilities, and interstate coordination almost instantly.
previous coverage of US quarantine policy after Covid
Why This Hantavirus Case Matters Beyond the Ship
Andes hantavirus remains rare in North America. But rarity does not reduce institutional pressure when fatality concerns enter the equation.
On 14 May 2026, the World Health Organization confirmed 11 cases tied to the Hondius outbreak, although Kornfeld’s negative PCR result may lower that figure after further review. According to the CDC, health officials now monitor exposed individuals for up to 42 days because symptoms can emerge weeks after transmission.
That timeline changes the burden.

Short quarantines disrupt schedules. Six-week monitoring periods reshape lives. Families delay travel plans. Workers pause contracts. Universities reconsider exposure protocols. Quietly.
Dr. David Fitter, incident manager for the CDC hantavirus response, said federal agencies continue working with passengers on “the best possible place” for monitoring. That language matters. It reflects a system trying to persuade rather than compel.
CDC hantavirus guidance and monitoring protocols
Side A: Precautions Protect Public Health
Public health officials argue the current approach follows established infectious disease logic.
Testing asymptomatic individuals too early can produce misleading results. Broad screening during incubation windows may create false reassurance and weaken monitoring discipline. That concern shaped the CDC’s decision to recommend testing primarily for symptomatic passengers.
Specialised centres like the University of Nebraska Medical Center and Emory University also provide something most hospitals cannot: high-containment infrastructure and trained infectious disease teams.
The system learned hard lessons during COVID. Rapid isolation, layered surveillance, and coordinated communication now form the backbone of outbreak management.
Officials want containment before escalation.
Side B: Extended Monitoring Erodes Public Trust
Passengers experience something different.
A person without symptoms can still lose freedom of movement for weeks because exposure alone carries institutional weight. That creates friction between individual autonomy and precautionary containment.
The gap between official reassurance and lived uncertainty grows fast during prolonged observation periods. One negative test no longer restores confidence psychologically. It simply opens another phase of waiting.
Again.
Public memory shapes this response as much as microbiology does. After years of pandemic restrictions, many Americans now measure public health credibility through consistency, transparency, and visible evidence.
Mixed international approaches complicate that trust further. Some countries tested all exposed passengers. US agencies chose selective testing instead.
WHO outbreak updates on Andes hantavirus
The Tension Inside Containment Medicine
The Hondius incident exposed a healthcare system that now operates in “probability mode.”
Hospitals and regulators increasingly respond to what might happen, not only what has happened already. That approach improves outbreak prevention. It also expands the social footprint of medical authority into travel, work, and personal movement.
Containment medicine no longer lives only inside hospitals.
It follows people home.
analysis of global disease surveillance systems
What Health Officials Watch Next
Over the next six to twelve months, health agencies will likely expand cruise-related infectious disease protocols.
Three developments matter most:
- Broader exposure-tracking systems for international travel
- More investment in regional biocontainment facilities
- Renewed legal debate over voluntary versus mandatory quarantine powers
The biggest indicator sits inside international coordination. If WHO members standardise hantavirus monitoring guidance, future outbreaks may trigger smoother cross-border responses. If countries continue with fragmented policies, travellers will face inconsistent testing, isolation, and reporting systems depending on where they land.
FAQ
What is Andes hantavirus?
Andes hantavirus is a rare virus linked to rodents and, unlike many hantavirus strains, can spread between people under certain conditions.
Why did passengers remain in quarantine after negative tests?
Health officials cited the virus’s long incubation period and the possibility of delayed symptom development.
How long does hantavirus monitoring last?
The CDC recommends monitoring high-risk exposures for 42 days after contact.
Why didn’t the CDC test every exposed passenger?
Officials said broad testing during incubation periods may produce unreliable or misleading results in asymptomatic individuals.
Which US hospitals handled the outbreak response?
The University of Nebraska Medical Center and Emory University managed specialised monitoring and containment operations.
AUTHOR BIO
Written by Elena Ward, a senior health systems analyst who has covered infectious disease policy, hospital preparedness, and global outbreak coordination for more than a decade.