

 English
English 



































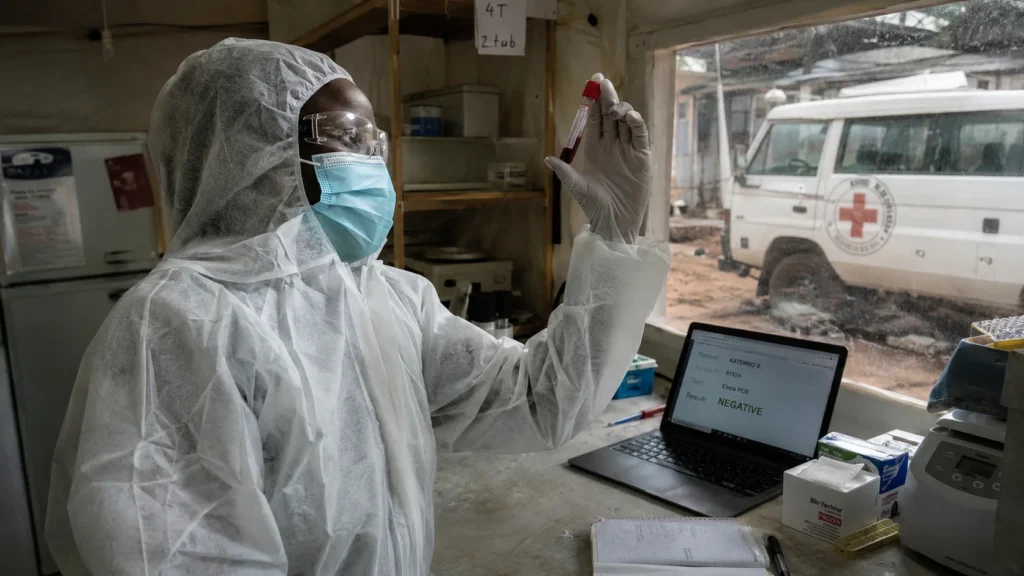










































































































































































































































The Ebola Test Was Negative. The Species Was Different.
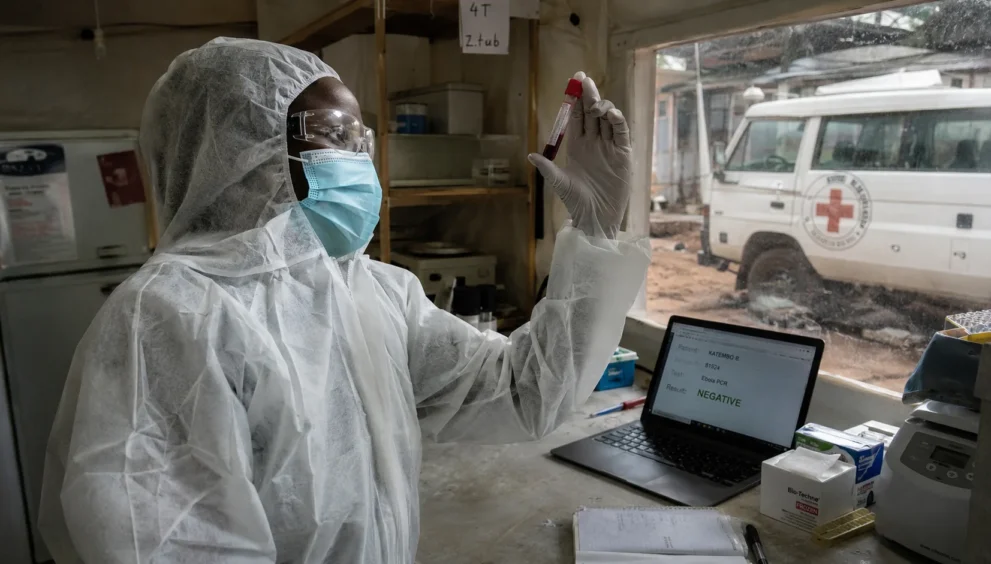
The nurse developed symptoms on 24 April. Fever, headache, tiredness—the presentation looked like malaria, like flu, like a dozen things that are not Ebola. The initial blood test came back negative. It was designed to detect the Zaire species, the most common strain. The virus in the nurse’s blood was Bundibugyo, a species that had not been seen for over a decade. The test could not find what it was not built to find. By the time anyone understood what they were dealing with, the nurse was dead, the body had been repatriated to Mongbwalu, and the funeral had exposed a number of people large enough to seed an outbreak.
The World Health Organization has now declared the outbreak a public health emergency of international concern. As of 11 June, the Democratic Republic of Congo has confirmed 689 cases and 139 deaths. The numbers are lower than earlier reports because many suspected cases have since tested negative. Thirty-two people have recovered. Five health workers are among the dead. Uganda has confirmed two deaths and 19 cases. Rwanda has closed its borders with the DRC. The epicentre is Ituri province, a conflict zone where a quarter of a million people are displaced, and territory changes hands between armed groups. The roads are bad. The vaccine for this species does not exist. The experimental drug being considered, obeldesivir, was developed for COVID. No one knows if it will work against Bundibugyo.
This is not an isolated event. This is a structural shift in what it means to confront an Ebola outbreak in a world that has learned to expect vaccines and rapid diagnostics—and is now discovering that those tools were built for a different virus.
The Diagnostic Gap
The first blood tests in the affected areas were negative. The tests were not faulty. They were specific. They had been designed to identify the Zaire species of Ebola, which caused the 2014-16 West African epidemic that killed more than 11,000 people and the 2018-20 outbreak in eastern DRC that infected more than 3,400. The global health infrastructure built after those outbreaks—the rapid tests, the vaccine stockpiles, the treatment protocols—was optimised for Zaire. It was not optimised for Bundibugyo.
Bundibugyo is rare. It has caused only two previous outbreaks: in 2007, when it was first detected in a district of Uganda that gave it its name, and in 2012. It kills about a third of those infected, less than Zaire, which has a case fatality rate of roughly 66%, and Sudan, at around 48%. The lower lethality is epidemiologically perverse: people live longer, infect more contacts, and die at rates still high enough to devastate communities.
The diagnostic delay was not a technical failure. It was a structural one. The tests were deployed based on assumptions about which virus was most likely. The assumptions were reasonable. The consequences were lethal. By the time Congolese health authorities had established four laboratories in Ituri—in Bunia, Mongbwalu, Beni, and Aru—capable of testing for Bundibugyo and delivering results within 24 hours, the virus had been spreading undetected for weeks.
The Vaccine That Does Not Exist
There is no approved vaccine for Bundibugyo. The Ervebo vaccine, which proved highly effective against the Zaire species during the 2018-20 outbreak, uses a vesicular stomatitis virus vector engineered to express a Zaire Ebola glycoprotein. It is species-specific. It does not target Bundibugyo. It is possible that it may offer some cross-protection. Nobody knows how much. The possibility is being investigated. The outbreak is ongoing.
Experimental vaccines for Bundibugyo are in development. Development is not deployment. The gap between a vaccine candidate and a vaccine in arms is measured in months at best, years more typically. The WHO has recommended evaluating obeldesivir, an experimental antiviral developed during COVID, under strict protocols to see whether it can prevent illness in people exposed to Ebola patients. The drug was designed for a coronavirus. It is now being tested against a filovirus. Science is adaptive. The adaptation takes time.
The absence of a vaccine changes the containment arithmetic. During the 2018-20 Zaire outbreak in eastern DRC, ring vaccination—immunising contacts of confirmed cases and contacts of contacts—helped limit transmission even in areas affected by conflict. That tool is not available here. The outbreak must be contained with the tools that exist: surveillance, contact tracing, isolation, safe burials, and public health communication. These are the tools that contained Ebola outbreaks before vaccines existed. They work. They work more slowly.
The Conflict That Contains the Response
Ituri province is a conflict zone. A quarter of a million people are displaced. Armed groups contest territory. Trish Newport, from Doctors Without Borders, told the BBC that the area changes hands so frequently that emergency response teams cannot simply drive to Ebola hotspots. A 90-kilometre journey from Bunia to Mongbwalu, one of two gold-mining towns where the majority of cases have been reported, takes more than three hours on bad roads. The roads do not improve when the security situation deteriorates.
The AFC-M23 rebel alliance, which controls parts of North Kivu and South Kivu, says it has established an Ebola response team. On 17 May, spokesman Lawrence Kanyuka said the group had “immediately activated” response mechanisms. Neither the government nor the rebels has explicitly said whether they are prepared to work together. Caitlin Brady, country director for the Danish Refugee Council, told the BBC that health officials and healthcare workers stayed and continued working after rebels seized Goma, meaning “the capacity to respond has remained.” The capacity is fragile. The cooperation is unstated. The virus does not negotiate.
The security situation compounds the epidemiological one. Contact tracing requires access. Access requires safe passage. Safe passage requires agreements between parties that are shooting at each other. The agreements may hold or they may not. The tracing continues either way.
The Funeral Problem
Congolese Health Minister Samuel Roger Kamba identified one reason the virus spread quickly: the number of people exposed to the body during the nurse’s funeral ceremony. This is not new. Ebola has always exploited the intimate rituals of death—the washing of bodies, the gathering of mourners, the contact between the living and the deceased that transmits the virus in its most concentrated form. Africa CDC director Dr Jean Kaseya told the BBC that funerals remain a particular concern.
Public health campaigns are now providing information on safe burial practices. The message is medically sound. The message is culturally difficult. Funerals are not medical events. They are social, spiritual, and familial. To tell communities that they cannot touch their dead is to ask them to suspend the most fundamental rituals of grief. The suspension is necessary. The necessity does not make it easy.
Kamba also noted delays in reporting cases because some communities believe the disease to be “witchcraft” or a “mystical illness.” People sought treatment from prayer centres and witchdoctors rather than hospitals. The belief is not irrational. It is a response to a disease that appears without warning, kills without explanation, and for which, in the Bundibugyo strain, there is no vaccine and no approved treatment. The official health system offers isolation and supportive care. The prayer centre offers meaning. The choice, for some, is not between science and superstition. It is between two systems of explanation, neither of which can guarantee survival.
Who Gains, Who Loses
The power recalibration is visible across multiple axes.
The WHO gains authority through the emergency declaration, which mobilises funding and focuses international attention. The declaration does not guarantee containment. It guarantees that the world is now watching.
Africa CDC gains a mandate and a budget—$319 million announced, with South African President Cyril Ramaphosa pledging an initial $5 million. The institution built to coordinate the continent’s response to health emergencies now faces a test of its operational capacity in a conflict zone with a rare viral strain.
The Congolese government gains international support and loses domestic credibility with communities that do not trust the official health system. The gap between the government’s epidemiological strategy and the community’s lived experience is the gap where transmission continues.
Patients and health workers lose the most. Five health workers are dead. Thirty-two people have recovered. The recovery number is small because the outbreak is still escalating. The case count will rise. The death count will rise. The health workers who continue to show up in facilities with no vaccine, no approved treatment, and uncertain security—are absorbing a risk that no protocol can fully mitigate.
Neighbouring countries lose freedom of movement. Rwanda closed its borders with the DRC. Uganda suspended flights, buses, and public transport crossing the border. President Yoweri Museveni postponed the Martyrs’ Day pilgrimage, a Christian holiday that usually draws thousands of Congolese nationals. The economic cost is secondary to the health cost. It is not zero.
The 12-Month Trajectory
The outbreak will continue to escalate before it peaks. The combination of a rare viral strain with no vaccine, a conflict zone with restricted access, and communities with limited trust in the official health system is the worst-case configuration for Ebola containment. The WHO emergency declaration will accelerate funding and deployment of resources. It will not resolve the structural problems.
The experimental vaccine pipeline will be tested. If a Bundibugyo candidate moves quickly through early trials, it could be deployed under emergency use protocols. If not, the outbreak will be contained with the tools that existed before vaccines—surveillance, isolation, safe burials—and the containment will take longer.
The obeldesivir trial will produce data. If the drug works, it will become the first approved treatment for Bundibugyo. If it does not, the standard of care will remain supportive treatment: fluids, electrolytes, oxygen, and time. Survival will depend on the quality of care available and the speed with which patients reach it. The quality is variable. The speed is often slow.
The political situation in eastern DRC will determine whether the health response can function. The rebels have signalled cooperation. The government has not confirmed it. The virus will exploit any gap between the two.