

 English
English 




















































































































































































































































































































































DR Congo Ebola Outbreak Declared Emergency With No Vaccine

Published: 17 May 2026 | Source: WHO Emergency Committee, Geneva
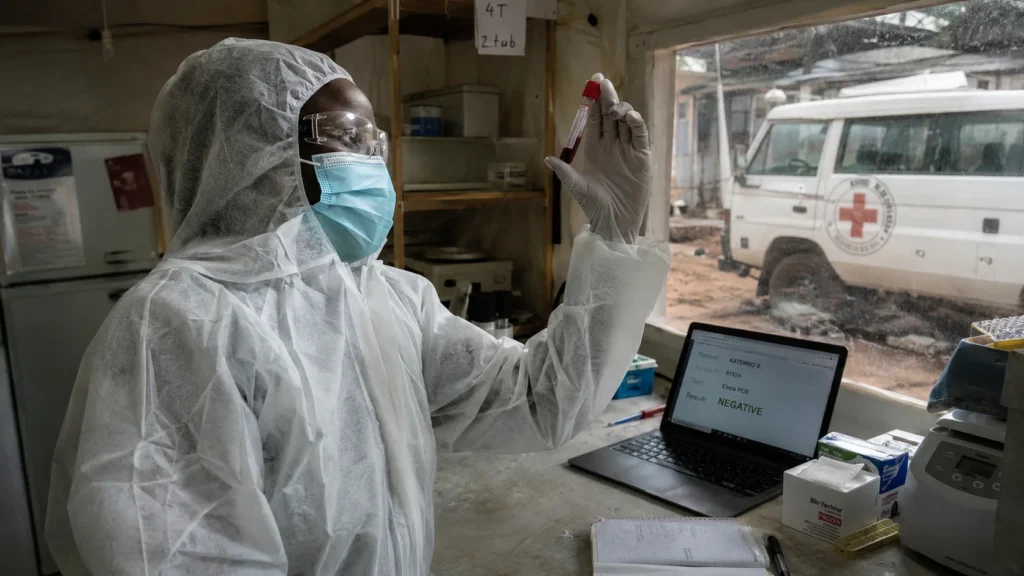
KINSHASA, DR CONGO — The DR Congo Ebola outbreak declared emergency by the World Health Organization this week, confronts a stark reality: the Bundibugyo strain driving it has no approved vaccine, no proven antiviral treatment, and has already spread from the gold-mining zones of Ituri province to the capital Kinshasa and across the border into Uganda. Around 246 suspected cases and 80 deaths have been recorded. The true numbers, the WHO warns, remain unknown.
What Is the Bundibugyo Ebola Strain?
Ebola is not a single virus. Three species cause human outbreaks. The Zaire strain — responsible for the 2018-2020 epidemic in eastern DR Congo that killed nearly 2,300 people — has approved vaccines. The Bundibugyo strain, first identified in Uganda in 2007, does not.
According to WHO disease outbreak news, May 2026, the Bundibugyo virus carries an average fatality rate of approximately 30% based on prior outbreaks. Early symptoms — fever, muscle pain, fatigue, headache, sore throat — mirror malaria and typhoid, diseases common in the mining communities where this outbreak began. Vomiting, diarrhoea, and haemorrhaging follow as the disease progresses.
Transmission occurs through direct contact with infected bodily fluids such as blood and vomit. The incubation period ranges from two to 21 days after infection.
Why the global vaccine pipeline keeps missing African Ebola strains
Where Has the Virus Spread?
The WHO confirmed eight laboratory-confirmed cases as of 17 May 2026, with suspected cases and deaths across three health zones: Bunia, the capital of Ituri province, and the gold-mining towns of Mongwalu and Rwampara.
One case reached Kinshasa — a returning traveller from Ituri. A laboratory in Goma, a city of two million currently under M23 rebel control, confirmed another case, AFP reported on Sunday AFP report, Goma confirmed case, May 2026.
Uganda confirmed two cases. A 59-year-old Congolese man died on Thursday and tested positive posthumously. Ugandan officials said his body was repatriated to DR Congo. The DR Congo Ebola outbreak declared emergency, now spans two countries with significant cross-border trade and population movement.
Why This Outbreak Differs From Previous Ones
Dr Tedros Adhanom Ghebreyesus, WHO director-general, warned of “significant uncertainties to the true number of infected persons and geographic spread.” That phrasing signals a surveillance gap. In a region where M23 rebels control Goma, mining militias operate in Ituri, and informal healthcare providers serve remote populations, the official case count is an undercount by definition.
Africa CDC executive director Dr Jean Kaseya flagged the urban settings of Rwampara and Bunia, plus mining activity in Mongwalu, as accelerants. “Significant population movement” between affected areas and neighbouring countries, he said, made regional coordination essential.
The WHO advised DR Congo and Uganda to establish emergency operations centres for monitoring, tracing, and infection-prevention measures. Confirmed cases should face immediate isolation and treatment until two Bundibugyo-specific tests conducted at least 48 hours apart return negative.
But here’s the operational reality: isolation protocols designed in Geneva operate differently in Mongwalu, where a miner’s household may rely on an informal clinic with no testing capacity.
How armed conflict in eastern DRC became a permanent epidemiological risk
The Economic and Trade Dimension
The WHO advised countries outside the affected region against closing borders or restricting travel and trade. Such measures, the agency said, “are usually implemented out of fear and have no basis in science.”
The advice is scientifically sound. Historically, it fails. West African states closed their borders during the 2014 outbreak. Countries worldwide imposed travel bans during COVID-19. Governments routinely subordinate epidemiological guidance to sovereign reflex.
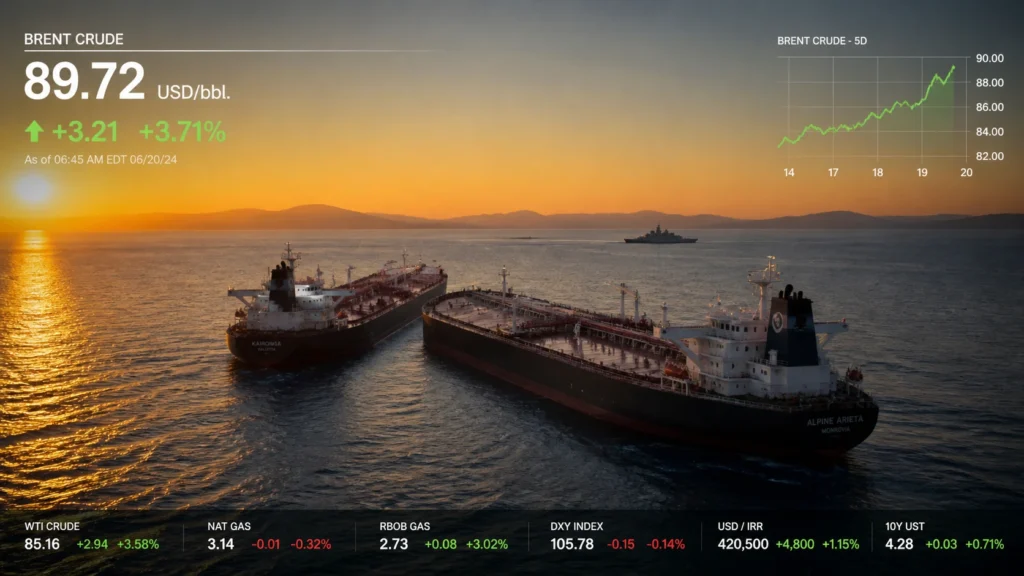
Markets already price the divergence. Insurance premiums for cargo moving through Entebbe, Kisangani, and the Great Lakes region will recalibrate. Mining operations in Ituri — gold, coltan, tin — face operational friction. The DR Congo Ebola outbreak declared emergency arrives alongside a separate geopolitical shock in the Strait of Hormuz that has already disrupted global shipping. Simultaneous systemic shocks compound. Institutions still model them in separate silos.
FAQ: DR Congo Ebola Outbreak 2026
What strain of Ebola is causing this outbreak?
The Bundibugyo virus was first discovered in Uganda in 2007. It differs from the Zaire strain that caused the 2018-2020 epidemic. There are no approved vaccines or antiviral drugs for Bundibugyo.
How many people have died so far?
Around 80 deaths have been reported from approximately 246 suspected cases across Ituri province, with one confirmed case in Kinshasa and two confirmed cases in Uganda. The WHO warns the true numbers are likely higher.
How does Ebola spread?
Through direct contact with infected bodily fluids such as blood, vomit, and diarrhoea. The incubation period is two to 21 days. Symptoms start with fever, muscle pain, fatigue, and headache before progressing to vomiting and haemorrhage.
Why is this outbreak considered high-risk?
The combination of active armed conflict in eastern DR Congo, high population mobility, urban transmission zones including Goma and Kinshasa, widespread informal healthcare, and the absence of an approved vaccine for this strain.
Has Uganda closed its border with DR Congo?
Not yet. The WHO advised against border closures. Ugandan authorities confirmed two cases, including one fatality, and repatriated the body. Border screening may intensify without formal closure declarations.
What to Watch in the Coming Months
The trajectory points toward sustained, under-measured transmission rather than rapid containment or catastrophic spread. Three indicators matter most.
First, the case count in Goma. One confirmed case in a rebel-held city of two million signals undetected transmission chains. Second, Uganda’s de facto border policy — whether authorities maintain open borders or quietly implement screening that becomes an effective restriction. Third, whether any major pharmaceutical regulator announces a fast-track pathway for a Bundibugyo vaccine. That would signal the Global North has recalculated its own exposure. So far, silence.
The gold mines are still operating. The cross-border traders are still moving. The incubation period is up to 21 days. Watch.
The global health security gap: why pathogen funding follows television cameras, not risk
Written by the Foreign Desk, drawing on WHO emergency committee statements, Africa CDC operational briefings, and institutional coverage of Ebola outbreaks dating to the 2014 West African epidemic. The desk has covered infectious diseases and health security for over 15 years.