

 English
English 



















































































































































































































































































































































How Outbreak News Warps Your Brain—Even If You’re Not Infected

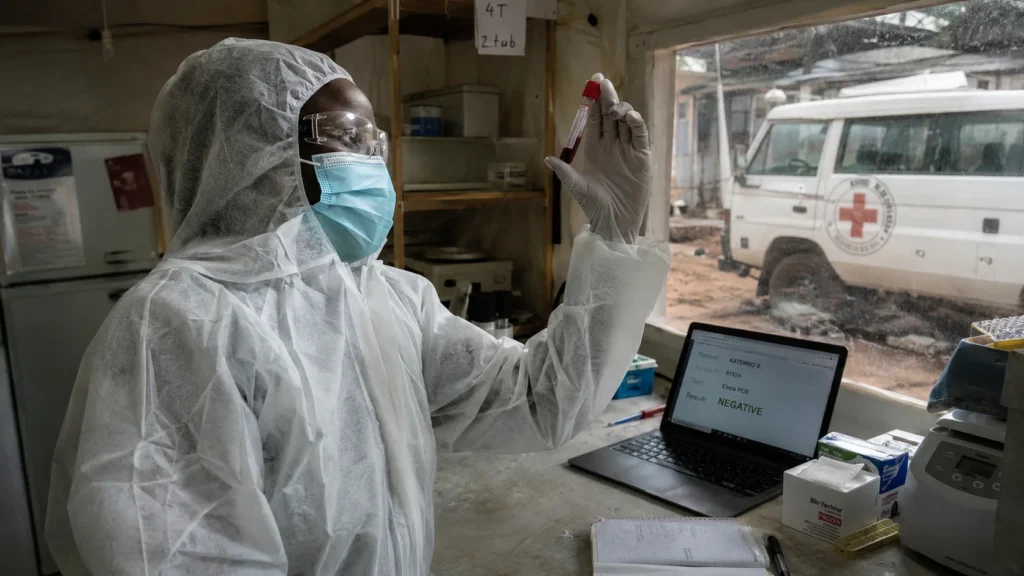
The Ebola outbreak in the Democratic Republic of Congo is escalating. Case counts are rising. Response efforts are falling behind. Most people reading this will never come into contact with the pathogen. They are thousands of miles from the outbreak zone. Their bodies require no immunological defence. Their minds are mounting one anyway.
The mechanism is called the behavioural immune system, a concept developed by Mark Schaller at the University of British Columbia. It is not a metaphor. It is a set of psychological responses that evolved to reduce contact with pathogens before they enter the body. The physical immune system is expensive to run. Activating macrophages, B-cells, and T-cells consumes enormous energy. The body would prefer not to need them. The behavioural immune system is the first line of defence. It operates on cues, not on infections. It activates at the suggestion of disease, not at the presence of it. The news you read about an outbreak thousands of miles away is a cue. Your brain responds as if the threat were nearby. The response is unconscious. The consequences are social.
This is not a psychology explainer. This is an Individual Liberty vs Public Health collision—a biological mechanism that evolved to protect individuals from infection now shaping how entire populations react to news of disease, with consequences for political attitudes, social cohesion, and the treatment of outsiders that public health agencies have not begun to account for.
The Mechanism: What Activates When Disease Is in the Headlines
The behavioural immune system’s most basic output is disgust. The smell of rotting food. The sight of open wounds. The body recoils before the brain has time to reason. The recoil is not learned. It is inherited. It is the same mechanism that makes you retch at the smell of spoiled meat. It is the same mechanism that activates when you read about an Ebola patient’s symptoms in a news article. The pathogen is not present. The cue is. The response is the same.
Beyond disgust, the system produces subtler effects. It increases conformity. In an experiment by Schaller, students who had just recalled a time when they had been sick were far more likely to vote in line with their peers on a proposed change to the school’s grading system. A separate study at the University of Hong Kong found that participants exposed to graphic images of open wounds and maggots—cues of infection—were more likely to follow the crowd when evaluating modern art. Participants who viewed images of car accidents, which are distressing but carry no infection risk, did not show the same conformity effect.
The evolutionary logic is straightforward. Cultures develop rules to reduce the spread of disease—hygienic food preparation, waste disposal, quarantine practices. In times of outbreak, adherence to those rules becomes more important. The behavioural immune system enforces adherence by making people more likely to follow social norms and more likely to judge harshly those who break them. Studies have shown that reminders of illness make people harsher in their moral judgements. Participants who had been primed with disease cues judged a couple more severely for having sex on the man’s grandmother’s bed. The behaviour is not rational. It is evolutionarily programmed. The programming does not distinguish between a real outbreak and a news story about one.
The Outsider Effect: How Disease Fear Fuels Xenophobia
Lene Aarøe and colleagues at Aarhus University in Denmark have produced a series of studies suggesting that the behavioural immune system causes people to “unconsciously tag immigrants as bearers of pathogens.” The tagging is not conscious. It is not reasoned. It is a byproduct of a system that evolved to treat unfamiliar people as potential sources of unfamiliar diseases. In ancestral environments, this was adaptive. Outsiders carried novel pathogens to which the local population had no immunity. Avoiding outsiders reduced the risk of infection. The mechanism has not updated for the era of global travel and modern epidemiology.
During the Covid-19 pandemic, Giulia Fuochi at the University of Padova in Italy and colleagues surveyed 685 Italians in April and May 2020. They found a significant correlation between people’s fear of the virus and their distrust of various minorities, including immigrants, drug-using adults, and foreign nationals. The mechanism was not direct. It operated through a weaker sense of shared identity and common destiny. The behavioural immune system was not making people hate outsiders. It was making people feel less connected to them. The distinction matters for understanding the effect. It is not that disease cues make people actively hostile. It is that they make people withdraw from those they perceive as different. The withdrawal is unconscious. The political consequences are real.
The effect is not uniform. Some people are naturally more fearful of disease and react more strongly to cues of infection. Others are less easily swayed. Personality, education, profession, family background, and personal experience all modulate the response. The behavioural immune system is not destiny. It is a pressure. The pressure can be resisted. It can also be amplified by political leaders who use disease fear to justify exclusionary policies. The outbreak news provides the cue. The political context determines what happens next.
The Limits of Laboratory Findings
The real-world evidence for the behavioural immune system is messier than the laboratory studies. Attempts to replicate the findings during actual outbreaks have produced mixed results. The Covid-19 pandemic provided a natural experiment, and one review noted changes in “social trust, interpersonal wariness, xenophobia, moral vigilance and political ideology” during the worst months. But other studies failed to find consistent effects. The messiness is not a refutation of the theory. It is a reminder that human behaviour is multiply determined. A news story about Ebola does not act on a blank slate. It acts on a person with a specific history, a specific personality, a specific set of relationships, and a specific political context. The behavioural immune system is one influence among many. It is not always the decisive one.
The distinction matters for public health communication. If disease news predictably increases xenophobia, public health agencies need to account for that when communicating about outbreaks. If the effect is real but weak and easily overridden by other factors, the communication challenge is different. The science is not settled. The precautionary principle suggests treating the effect as real until the evidence is clearer. The cost of ignoring it is the unnecessary amplification of social divisions during outbreaks. The cost of overstating it is the unnecessary pathologising of normal responses to frightening news.

Power Recalibration: Who Gains, Who Loses
Public health agencies gain a communication challenge they have not fully absorbed. The behavioural immune system means that outbreak communication is not neutral. The words and images used to inform the public also activate psychological responses that can increase prejudice and social division. The agencies that communicate about Ebola and hantavirus are not just conveying epidemiological information. They are activating an ancient psychological system with predictable social consequences. The system needs to be accounted for in communication strategies. It currently is not.
Political actors who benefit from xenophobia gain an activation mechanism they can exploit. Disease fear is a resource. Leaders who want to increase distrust of outsiders can amplify disease cues. The amplification does not need to be explicit. It can operate through the selection of which outbreaks to cover, which images to show, and which language to use. The behavioural immune system does the rest.
Immigrants and minority groups lose from the activation of a system that tags them as pathogen risks. The tagging is unconscious. The consequences are not. During outbreaks, hostility toward outsiders increases. The increase is measurable. The people affected are real.
The public loses the ability to distinguish between rational disease prevention and irrational fear. The behavioural immune system operates on cues, not on risk assessments. A news story about Ebola in DR Congo activates the same psychological response as a local outbreak. The system does not know the difference. The public, unless educated about the mechanism, does not know the difference either.